Healthcare delivery in England is undergoing structural transformation. Integrated Care Systems, neighbourhood health models, and cross-sector collaboration between NHS services, social care, community providers, and independent sector partners are becoming central to service delivery. These reforms are designed to improve continuity of care, reduce fragmentation, and support earlier intervention closer to patients' homes.
These ambitions introduce a structural challenge that is less visible than workforce capacity or funding pressure, but equally fundamental. As care becomes more collaborative, responsibility becomes more distributed. Clinical decisions increasingly rely on information, workflow coordination, and accountability signals that cross organisational boundaries. The digital infrastructure supporting these interactions has historically focused on data sharing and workflow coordination. It has paid less attention to preserving governance continuity when care crosses those boundaries.
Inference Clinical has developed Governance Core to address this problem directly. Governance Core is not a clinical system, an integration engine, or a workflow platform. It is an enforcement layer designed to ensure that responsibility, consent, and evidence integrity remain visible, attributable, and reconstructable as patients move between organisations, care settings, and digital services.
Integration Changes Where Risk Lives
Integration programmes are often framed as coordination challenges. In practice, they are accountability challenges.
In traditional single-provider models, responsibility is relatively stable. When care expands across primary care networks, community providers, acute trusts, social care services, digital triage platforms, and independent providers, responsibility becomes dynamic. Responsibility is accepted, shared, transferred, and relinquished under different conditions and over different timeframes.
Clinicians working across these environments frequently experience the operational consequences of this complexity. Referral pathways may involve multiple services interpreting consent differently. Monitoring responsibilities may be assumed informally rather than explicitly accepted. Information may arrive in clinical systems without clear provenance or contextual safeguards that explain how it should be interpreted. When adverse events occur, investigations often focus on individual decision-making when the underlying failure relates to responsibility clarity or governance signal loss.
These challenges are increasingly recognised within national policy discussions around neighbourhood health and integrated care delivery. Delivering joined-up care requires organisations to collaborate operationally, but collaboration introduces new forms of risk when governance signals degrade as data and responsibility move between systems.
Governance as Infrastructure Rather Than Documentation
Healthcare governance traditionally relies on policy, protocol, and retrospective assurance. NHS organisations implement governance frameworks supported by professional standards, clinical safety case development under DCB 0129 and DCB 0160, and regulatory oversight mechanisms. These approaches are essential, but they assume that governance rules are preserved through organisational behaviour and documentation alone.
Modern digital healthcare operates across distributed systems, asynchronous workflows, and multi-organisational care pathways. In this environment, governance rules must be preserved in real time as operational properties of the infrastructure that supports care delivery.
Governance Core is designed around three structural requirements.
Responsibility must remain attributable throughout a care interaction, including the conditions under which responsibility is accepted and the timeframe for which it applies.
Consent must remain bound to purpose, participating organisations, and duration, ensuring that consent is not silently reinterpreted as data moves across services.
Clinical decision-making must remain reconstructable. When incidents occur, organisations must be able to determine what information was available, who acted on it, what governance rules applied, and what responsibilities were in force at the time.
These requirements are implemented as enforceable system behaviour rather than policy interpretation or retrospective audit reconstruction.
A Constitutional Model for Clinical Governance
Governance Core is built around a constitutional model. The constitution defines non-negotiable governance guarantees that must be preserved regardless of organisational complexity, digital transformation programme design, or integration architecture.
The constitutional guarantees enforced by Governance Core include responsibility attribution, consent boundary preservation, evidence integrity, identity continuity, and workflow context preservation. These guarantees are enforced through deterministic system behaviour rather than organisational expectation.
Governance Risk in Practice: Consent Drift Across Integrated Referral Pathways
Integrated Care Systems are designed to improve continuity of care by enabling patients to move more smoothly between services. Referral pathways increasingly involve multiple providers contributing to assessment, treatment, monitoring, and follow-up care. These pathways are essential to delivering coordinated neighbourhood care and reducing pressure on acute services.
However, integrated referral pathways introduce governance risks that are rarely visible during routine operation.
Consider a patient referred from general practice to a community musculoskeletal service. The patient provides consent for referral, assessment, and information sharing with the receiving service. During the course of assessment, the community service refers the patient onward to a specialist provider for diagnostic imaging. Imaging results are later reviewed by a virtual multidisciplinary team that includes clinicians from additional organisations.
At each stage, information is shared appropriately to support patient care. From an operational perspective, the referral chain appears to function successfully. The patient progresses through assessment and treatment without apparent delay.
The governance risk emerges in how consent is interpreted and preserved across each transition.
The patient's original consent may have been provided for referral to a specific service or defined clinical purpose. As referrals progress, downstream services frequently rely on upstream consent assumptions rather than verifying how consent was originally scoped. Over time, consent may be treated as general permission for participation in a pathway rather than contextual authorisation linked to defined services, purposes, and timeframes.
This form of consent drift is rarely intentional. It arises because digital referral and data exchange systems often prioritise information availability rather than consent lineage. Clinicians receiving referrals are expected to act on available clinical information, frequently without access to structured evidence describing how patient consent applies to their involvement.
When pathways function smoothly, consent drift remains invisible. When concerns arise, organisations may struggle to demonstrate how consent was interpreted across multiple providers. Clinical safety investigations, patient complaints, or regulatory reviews often reveal that consent boundaries were never preserved in a form that could be consistently interpreted by participating services.
Consent drift creates additional risks beyond lawful processing considerations. It can introduce uncertainty about clinical responsibility, particularly when monitoring or follow-up care responsibilities are assumed across organisational boundaries. Patients may reasonably believe they are under the care of a specific service, while operational responsibility has shifted to another provider without explicit confirmation or documented acceptance.
Governance Core preserves consent as contextual governance evidence rather than static access permission. The system maintains structured linkage between consent, participating organisations, clinical purpose, and timeframe. When referrals or responsibility transitions occur, governance signals remain visible and enforceable, reducing reliance on implicit interpretation.
Governance Risk in Practice: Responsibility Transfer in Distributed Monitoring
Neighbourhood and integrated care models increasingly rely on shared monitoring arrangements. Virtual wards, community follow-up pathways, and post-discharge monitoring services depend on coordinated responsibility across multiple providers.
Consider a patient discharged from an acute trust following treatment for heart failure. The discharge plan includes remote monitoring supported by a community nursing service, with escalation criteria defined for deterioration. The patient is also scheduled for review by their general practice team and may be under the oversight of a specialist outpatient service.
Operationally, this model supports early discharge, reduces hospital bed pressure, and allows monitoring to occur closer to home. Clinically, it requires clear responsibility acceptance across multiple organisations.
In practice, monitoring responsibility often emerges through workflow expectation rather than explicit acceptance. The acute service may assume that community monitoring has begun once discharge documentation is transmitted. Community services may assume that monitoring responsibility is shared until initial patient contact occurs. General practice teams may receive monitoring data or escalation alerts without clear definition of their operational responsibility within the pathway.
These ambiguities rarely cause immediate disruption. Monitoring may occur successfully, and escalation may be handled appropriately. The risk becomes visible when deterioration occurs during responsibility transitions or when multiple providers assume another organisation is providing active oversight.
Clinical incident reviews frequently reveal uncertainty around when responsibility transferred, who accepted monitoring accountability, and under what conditions responsibility should have reverted to another service. These ambiguities create clinical risk and expose clinicians and organisations to accountability uncertainty despite acting in good faith.
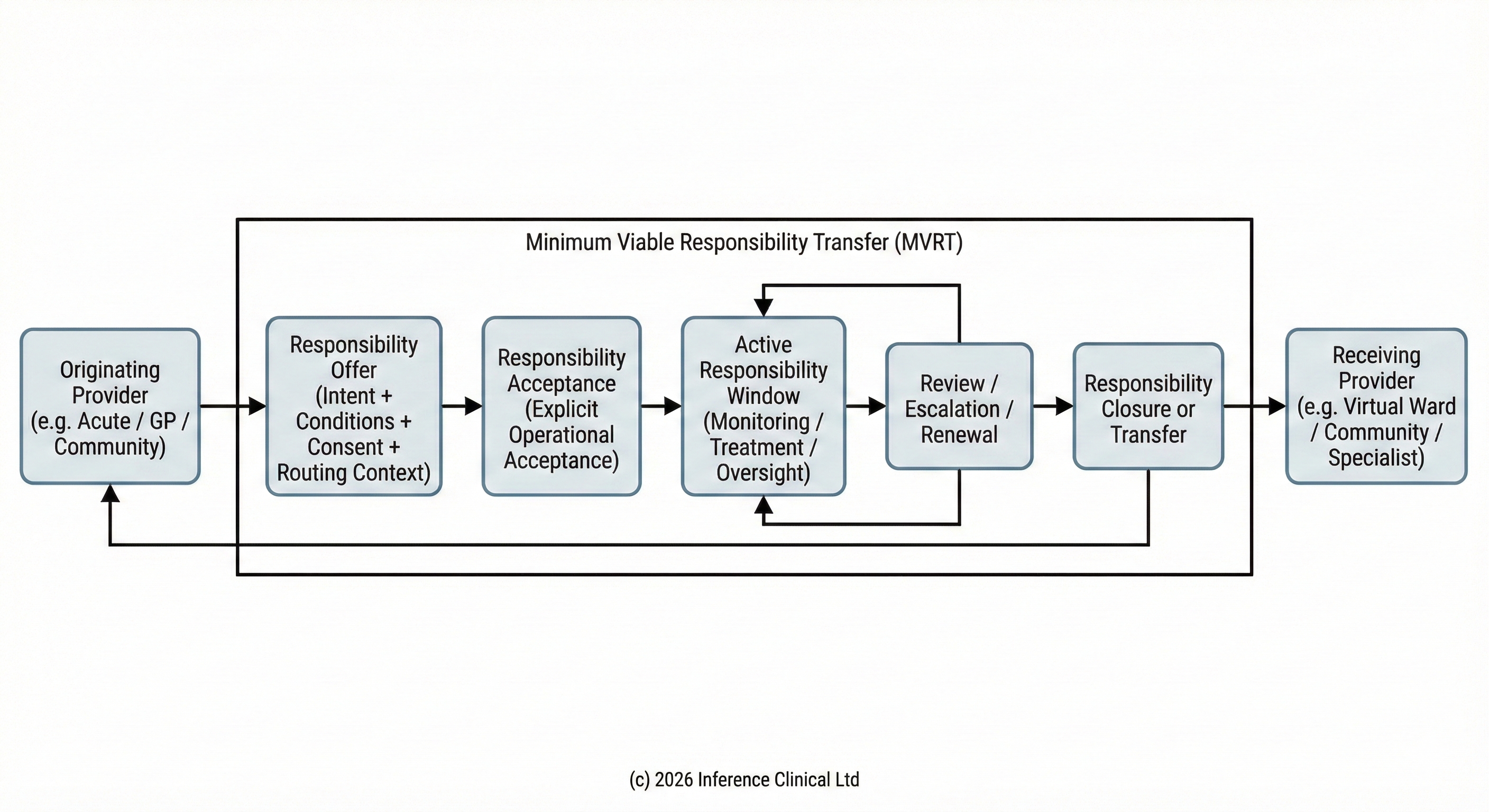
Governance Core introduces infrastructure designed to support explicit, condition-based responsibility acceptance and transfer. Responsibility transitions are recorded as defined operational events linked to conditions, timeframes, and participating services. Responsibility cannot exist in an implicit or assumed state. The system preserves evidence describing how responsibility was formed and under what conditions it changes.
This model provides infrastructure foundations for approaches such as Minimum Viable Responsibility Transfer, where responsibility is treated as a time-bounded, condition-based operational state rather than an organisational assumption. By making responsibility acceptance explicit and reconstructable, Governance Core supports safe distributed monitoring models and strengthens accountability clarity across neighbourhood care pathways.
Mechanical Enforcement and Clinical Safety Assurance
Governance Core enforces constitutional guarantees through deterministic system behaviour. Governance is implemented as operational infrastructure rather than advisory documentation.
Governance rules are enforced during system development through safety checks embedded within deployment pipelines. These checks ensure that software changes cannot introduce governance behaviour that violates safety invariants without traceability and review. This supports clinical safety assurance aligned with DCB 0129 and DCB 0160 responsibilities for manufacturers and deploying organisations.
During operational use, the system prevents governance actions from proceeding when identity, consent, responsibility, or evidence integrity conditions are unclear or invalid. The system is designed to fail in ways that preserve patient safety and accountability clarity rather than allowing governance ambiguity to persist silently.
Governance events are recorded in a form that supports independent clinical safety review, regulatory inspection, and organisational learning. This aligns with emerging expectations within NHS digital assurance frameworks and DTAC governance principles.
Supporting Neighbourhood Health and Integrated Care
Neighbourhood health models require services to collaborate around shared patient populations, often involving primary care, community services, social care, and voluntary sector partners. These models depend on distributed decision-making, shared monitoring responsibilities, and coordinated escalation pathways.
While these models improve care accessibility and continuity, they increase reliance on clear accountability boundaries. When responsibility is assumed informally or consent is interpreted inconsistently between services, patients can fall into gaps that are operationally invisible but clinically significant.
Governance Core provides infrastructure that makes accountability transitions explicit and enforceable. It supports organisations participating in integrated care by ensuring that responsibility acceptance, consent interpretation, and evidence preservation remain visible across organisational boundaries.
The Role of AI and Advisory Systems
Healthcare organisations are increasingly deploying AI-driven analytics, triage support, and risk detection capabilities. Governance Core enforces a strict separation between advisory intelligence and operational authority.
AI systems may identify risk signals, support clinical attention routing, or assist governance monitoring. They are not permitted to assign clinical responsibility, alter consent boundaries, authorise clinical decisions, or suppress governance evidence trails. This separation is enforced mechanically to support safe adoption of analytical technologies while maintaining clinical accountability and professional governance standards.
Relationship to NHS Clinical Safety and Regulatory Frameworks
Governance Core supports the construction of clinical safety cases aligned with recognised UK frameworks including DCB 0129 and DCB 0160. The system provides infrastructure that strengthens hazard traceability, governance evidence preservation, and safety case assurance activities.
The design also supports accountability requirements emerging within integrated care systems, collaborative commissioning under the Provider Selection Regime, and national policy emphasis on transparent and accountable data use across neighbourhood health delivery.
By embedding governance enforcement into infrastructure, Governance Core strengthens organisational ability to demonstrate compliance while reducing reliance on retrospective interpretation.
Scope and Limitations of Governance Core Version 1.0
Governance Core v1.0 is intentionally constrained. It does not automate clinical decision-making, replace clinical judgement, or define clinical pathways. It does not attempt to deliver interoperability independently of wider digital transformation architecture. Its purpose is foundational: to ensure that governance signals remain intact when care crosses organisational and technological boundaries.
Clinical Collaboration and Ongoing Development
Governance Core is designed to evolve through collaboration with clinicians, clinical safety officers, governance professionals, and regulatory stakeholders. Future development will include structured mechanisms allowing clinicians to challenge governance assumptions, identify operational failure modes, and contribute to refinement of enforcement safeguards.
Conclusion
Integrated care, neighbourhood health delivery, and digitally mediated clinical services are reshaping healthcare delivery across England. These developments improve continuity of care but increase reliance on infrastructure capable of preserving accountability across organisational boundaries.
Governance cannot remain solely documentary in distributed healthcare systems. Responsibility, consent, and evidence integrity must become enforceable properties of the infrastructure that supports care delivery.
Governance Core represents an attempt to provide infrastructure that preserves accountability clarity and clinical safety as healthcare delivery becomes increasingly collaborative, distributed, and digitally enabled.
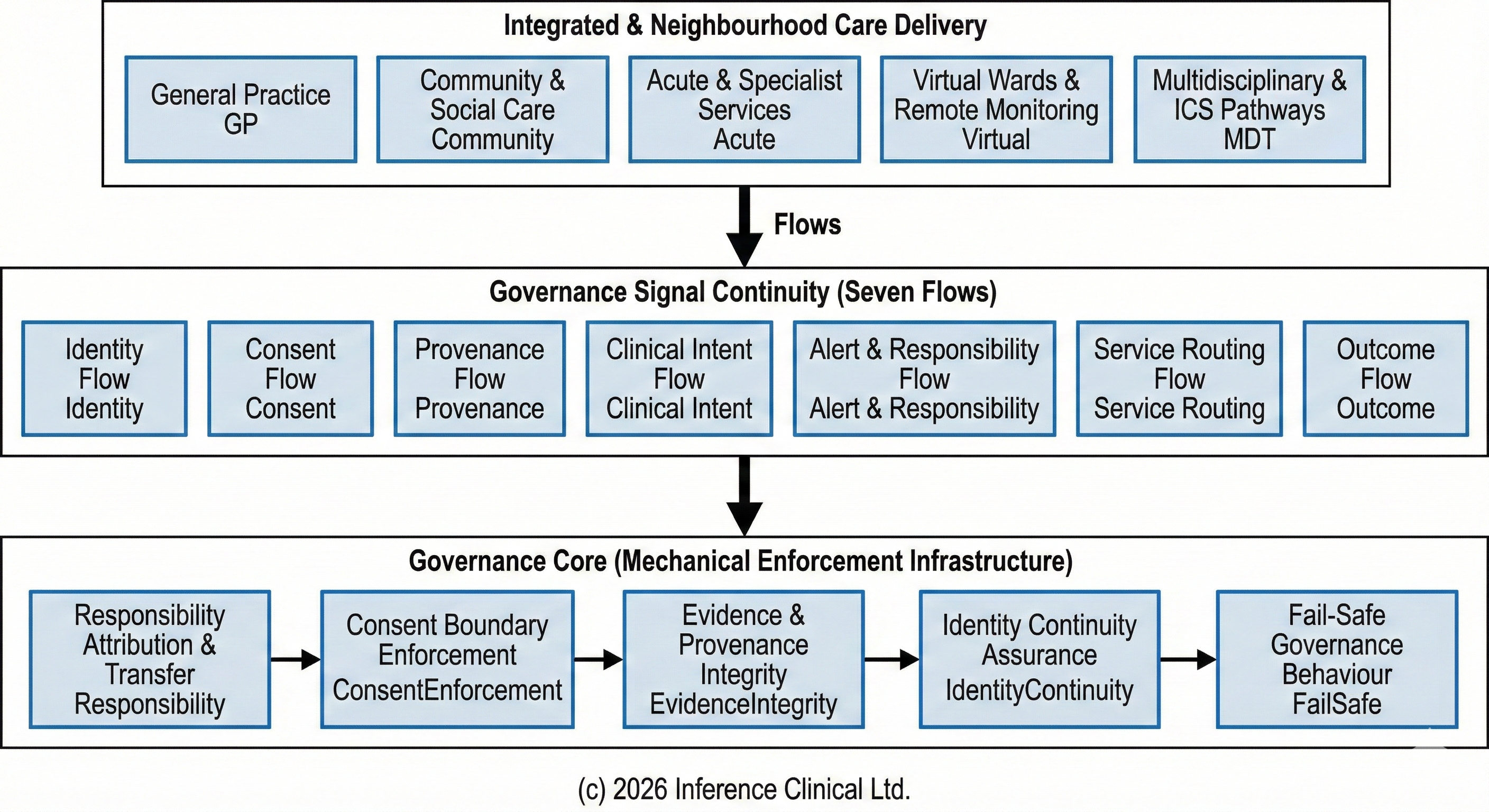
Governance Core as the Foundation for the Seven Flows Model
Governance Core represents the enforcement foundation upon which broader governance orchestration models can be safely developed. Within Inference Clinical's wider architectural framework, this enforcement layer supports the implementation of the Seven Flows model, which describes the core governance signals required to sustain safe, accountable care across organisational boundaries.
The Seven Flows model recognises that safe integrated care depends on the continuity of seven interdependent governance domains: Identity, Consent, Provenance, Clinical Intent, Alert and Responsibility, Service Routing, and Outcome. These flows describe how accountability signals must move alongside clinical data and operational decision-making as patients transition between providers, care settings, and digital services.
Without enforceable infrastructure, these governance signals frequently degrade as information crosses organisational or technological boundaries. Governance Core is designed to provide the mechanical enforcement layer that preserves these signals, ensuring that responsibility attribution, consent integrity, and evidence continuity remain intact as healthcare delivery becomes increasingly distributed.
This layered approach reflects a broader principle: integration without governance continuity introduces risk, even when data exchange and workflow coordination appear operationally successful. By establishing enforceable governance guarantees at infrastructure level, Governance Core provides a stable foundation upon which integrated care workflows, responsibility transfer models, and neighbourhood health delivery frameworks can safely evolve.
Further detail on the Seven Flows model and its role in enabling accountable, interoperable healthcare can be found in our overview of the Seven Flows governance framework.
