Where should I start?
Architecting Neighbourhood Health
The NHS neighbourhood health model multiplies organisational boundaries within a single building. Ten articles on governance infrastructure before centres open.
Start the series →CQC, PHIN & practising privileges
Governance failures at the boundary between private hospitals, insurers, and the NHS. From Paterson Inquiry lessons to CMA Order compliance.
Start reading →The Local Authority–NHS constitutional boundary
The most constitutionally complex crossing in English healthcare. Two legal domains, different regulators, shared populations — no governed crossing.
Start reading →Healthcare boundary governance
Why care fails between organisations, not within them. Boundary governance for ICS place-based partnerships, neighbourhood health, and provider collaboratives.
Start reading →Clinical Governance Between Private Healthcare Providers
CQC inspects your organisation. GMC regulates your consultants. FCA oversees your insurer. Each regulator examines the node. None of them examine the crossing. Four articles on what those ungoverned crossings cost.
View the seriesArchitecting Neighbourhood Health
The NHS neighbourhood health model multiplies organisational boundaries within a single building. Why co-location doesn't solve the governance problem — and what infrastructure is needed before centres open.
View the seriesPrivate Healthcare Governance
The Paterson Inquiry exposed what the sector already knew: governance fails at the boundary between organisations, not within them. From practising privileges to insurer networks, PE integration, and the consultant who works both sides.
View the seriesThe Local Authority–NHS Constitutional Boundary
The boundary between local authority social care and the NHS is the most constitutionally complex crossing in English healthcare. Two constitutional domains, different legislation, different regulators — sharing responsibility for the same populations with no governed crossing.
View the seriesHealthcare Boundary Governance
Why organisational boundaries are the blind spot in NHS reform, private healthcare governance, and clinical safety. Analysis of the structural gap that no existing framework addresses — and the methodology to close it.
View the seriesSafe Responsibility Transfers
Why clinical governance can't stay procedural — and what Minimum Viable Responsibility Transfer means for healthcare infrastructure. From design principles to system architecture.
View the seriesMind the Gap
Where clinical safety actually fails — and what infrastructure would make it safer. Exploring the structural gaps in healthcare handoffs, accountability, and care transitions.
View the seriesFrom Foundations to Governance
Your structured path through NHS digital health compliance. Six posts covering DCB0129, clinical safety cases, hazard management, and building governance that scales.
Start the series
The Coherence Problem: Why NHS Transformation Always Fails
The NHS doesn’t lack energy, talent, or ambition. It lacks coherence — the infrastructure that maintains stable relationships between organisations as care crosses boundaries. Physics explains why.
Safety Lives in the Transitions
Healthcare doesn’t fail where you’d expect it to. The pattern that drives avoidable readmissions is simpler and harder to fix — it happens in the spaces between organisations.
Why GP Data Sharing Keeps Failing — And What’s Actually Missing
The NHS has tried to centralise GP data four times in twelve years. Each attempt collapsed. Not because of technology or consent — because nobody built the governance infrastructure that data sharing requires.

Paper Governance is a Liability: Why Healthcare Information Governance Must Move to the Infrastructure Layer
DPIAs, DSPTs, and Data Sharing Agreements describe what organisations intend to do with data. They don’t enforce it. Documentation is not governance.
Why Patients Can’t Track Their NHS Referrals — And What Would Have to Change
Why the NHS e-Referral Service was never designed for patient visibility — and the governance infrastructure that would have to exist before transparent referral tracking becomes safe.

The Compliance Wall: Why Private Healthcare Providers Can No Longer Ignore Digital Infrastructure
Seven legislative instruments — from the Health and Care Act 2022 to the Cyber Security and Resilience Bill — now impose mandatory digital infrastructure obligations on every private healthcare provider in England. The era of optional compliance is over.

Cross-Organisational Clinical Governance: The Structural Risk No NHS Provider Model Has Solved
Every NHS provider model — digital front doors, corporate contract holders, clinician-led federations, scaled regional providers — converges on the same structural weakness: responsibility transfer between organisations.
What Stripe’s Ledger Teaches Us About Patients Falling Through the Gaps
Stripe tracks $1 trillion with 99.9999% explainability. The NHS tracks clinical responsibility transfer with approximately 0%. The engineering patterns to fix this already exist. They just haven’t been applied here yet.

The Handover Problem Nobody Has Solved
NICE told the NHS to use structured handovers. The evidence shows 91% error reduction within hospitals. But across organisational boundaries — where patients are most vulnerable — the infrastructure still doesn't exist.

PSIRF Has an Infrastructure Problem — And It’s Hiding in the Gaps Between Organisations
PSIRF got the philosophy right. But philosophy without infrastructure is aspiration. The infrastructure gap between organisations is where learning goes to die.

The NHS Cannot See Itself
The NHS's fundamental problem is flow. Not data, not apps, not platforms. It is a system structurally unable to observe itself at the points that matter most. And we are spending billions making the problem worse.
Engineering Clinical Handoffs: What Carrying My Own Notes Taught Me About Healthcare's Missing Infrastructure
A year ago I was a patient carrying my self-written clinical notes on an iPad between appointments. Today I'm building the infrastructure that should have made that unnecessary. This is what I learned about healthcare's seven broken flows.

Your Clinical Safety Framework Is Broken. And Nobody's Allowed to Say So.
The NHS has a clinical safety problem hiding inside an organisational culture problem. Psychological safety isn't an HR initiative — it's critical infrastructure for DCB 0129 compliance. The hierarchy is the hazard.

The API Illusion: Why Health Interoperability Is Stuck in Yesterday's Thinking
Twenty years of API-first thinking has produced technically connected but governmentally disconnected healthcare systems. The problem isn't the pipes — it's what we forgot to send through them.

What the National Neighbourhood Health Simulation Revealed About Responsibility at the Boundaries
The neighbourhood health model works. The simulation proved it. But when context fragments across well-intentioned services, a child can become vulnerable — and the system, despite its best efforts, may not see it.
The Missing Infrastructure Layer in NHS Neighbourhood Health
An analysis of the NNHIP Regional Learning Events. 940 practitioners across 43 place teams describe the same structural gap: inter-organisation responsibility transfer infrastructure. The Seven Flows framework maps directly to what they're asking for.

The Regulatory Convergence: Six Pressures Arriving at the Same Boundary
FCA Consumer Duty, CQC restructuring, MPAF, PHIN/CMA, HSSIB, and the DCB standards review — six regulatory pressures converging on the organisational boundary. The organisations that build boundary governance now will shape the standards rather than scramble to meet them.

The Seven Flows Applied to Insured Patient Pathways: A Boundary Governance Methodology
Seven governance questions at five boundary crossings. A 7×5 maturity matrix that makes the gap measurable. The methodology that connects every argument in this series — and provides the audit framework for closing the governance gap.

The Digital Front Door: Where a Clinical Consultation Becomes a Commercial Pathway and Nobody Governs the Crossing
Every major UK insurer now offers a virtual GP as the entry point to private healthcare. The consultation is clinically governed. The crossing from clinical care to commercial pathway is not. The one-way valve mapped against the Seven Flows.

The NHS-Private Interface: Two Constitutional Domains, One Patient, No Governed Crossing
Every privately treated patient crosses the NHS-private boundary at least twice. Neither domain was designed to interoperate. From prescribing walls to data governance asymmetry — the structural gap mapped against the Seven Flows.

The Clinical-Commercial Boundary: Where Medical Necessity Meets Policy Wording and Nobody Governs the Gap
The consultant recommends treatment. The insurer decides whether to authorise it. Between them sits a governance domain governed by neither CQC nor FCA — and where the Consumer Duty creates an accountability reckoning.

The Provider Network as Ungoverned Constellation: How Insurer Routing Creates Clinical Boundaries Nobody Governs
Bupa, AXA, Vitality, Aviva — four routing models, billions in premiums. Seven crossings in a typical insured pathway mapped against the Seven Flows. The GP boundaries broken in both directions, and why the FCA Consumer Duty changes the equation.

Practising Privileges, Provider Networks, and the Governance Gap Nobody Is Measuring
The Paterson Inquiry exposed what private healthcare already knew: governance fails at the boundary between organisations, not within them. From practising privileges to insurer networks, the CQC/FCA regulatory gap, and the four boundaries every patient pathway crosses.

Architecting for Neighbourhood Health: The Technology Pillar — Why Interoperability That Doesn’t Preserve Governance Is Interoperability in Name Only
The Technology pillar asks whether digital infrastructure enforces or merely enables the governance architecture defined by the preceding four pillars — identity verification, consent recording, provenance preservation, clinical intent, MVRT-capable responsibility tracking, and outcome communication.
Architecting for Neighbourhood Health: The People Pillar — Why Generic MDT Training Doesn’t Cross Organisational Boundaries
The People pillar asks whether clinicians who work at boundaries understand the governance architecture — legal literacy, clinical safety awareness, crossing choreography knowledge, and escalation competence developed per boundary, not as generic MDT training.

Architecting for Neighbourhood Health: The Process Pillar — Crossing Choreography and the Pre-Conditions Nobody Defines
The Process pillar asks what must each party confirm before this specific crossing can validly occur. Crossing type enumeration, pre-condition frameworks (sender, receiver, bilateral), escalation pathways, and informal crossing governance at every bilateral boundary.
Architecting for Neighbourhood Health: The Clinical Safety Pillar — When the Hazard Sits Between Organisations
The Clinical Safety pillar answers what goes wrong when a boundary crossing fails. DCB 0129 and DCB 0160 are scoped to single organisations — boundary hazards fall through the gap. Seven Flows hazard identification, cascade-adjusted scoring, and CSO coordination fill the space between hazard logs.
Architecting for Neighbourhood Health: The Legal Pillar — Data Sharing, Contractual Frameworks, and Constitutional Compliance
The Legal pillar answers one question: may this boundary crossing happen? Every cross-boundary data flow must satisfy UK GDPR and common law duty of confidentiality simultaneously. Without lawful DSAs, DPIAs, and Caldicott coordination, everything built on top is unlawful.

Architecting for Neighbourhood Health: Boundary Readiness — Why “People, Process, Technology” Fails at Healthcare Boundaries
PPT was designed for single-organisation transformation. The Boundary Readiness model replaces it with five pillars — Legal, Clinical Safety, Process, People, Technology — assessed in dependency order at every bilateral boundary.
Architecting for Neighbourhood Health: Constitutional Complexity — Five Organisations, Five Legal Frameworks, One Building
Five data controllers, at least three regulators, two employment models, one building. Co-location makes constitutional boundaries invisible to patients — it does not dissolve them.

Architecting for Neighbourhood Health: Clinical Responsibility Transfer — Why Handover Frameworks Don’t Cross Organisational Boundaries
SBAR, safety huddles, and surgical checklists were designed for handovers within organisations. MVRT is the principle for transfers between them — and the neighbourhood health model is about to test it at unprecedented scale.

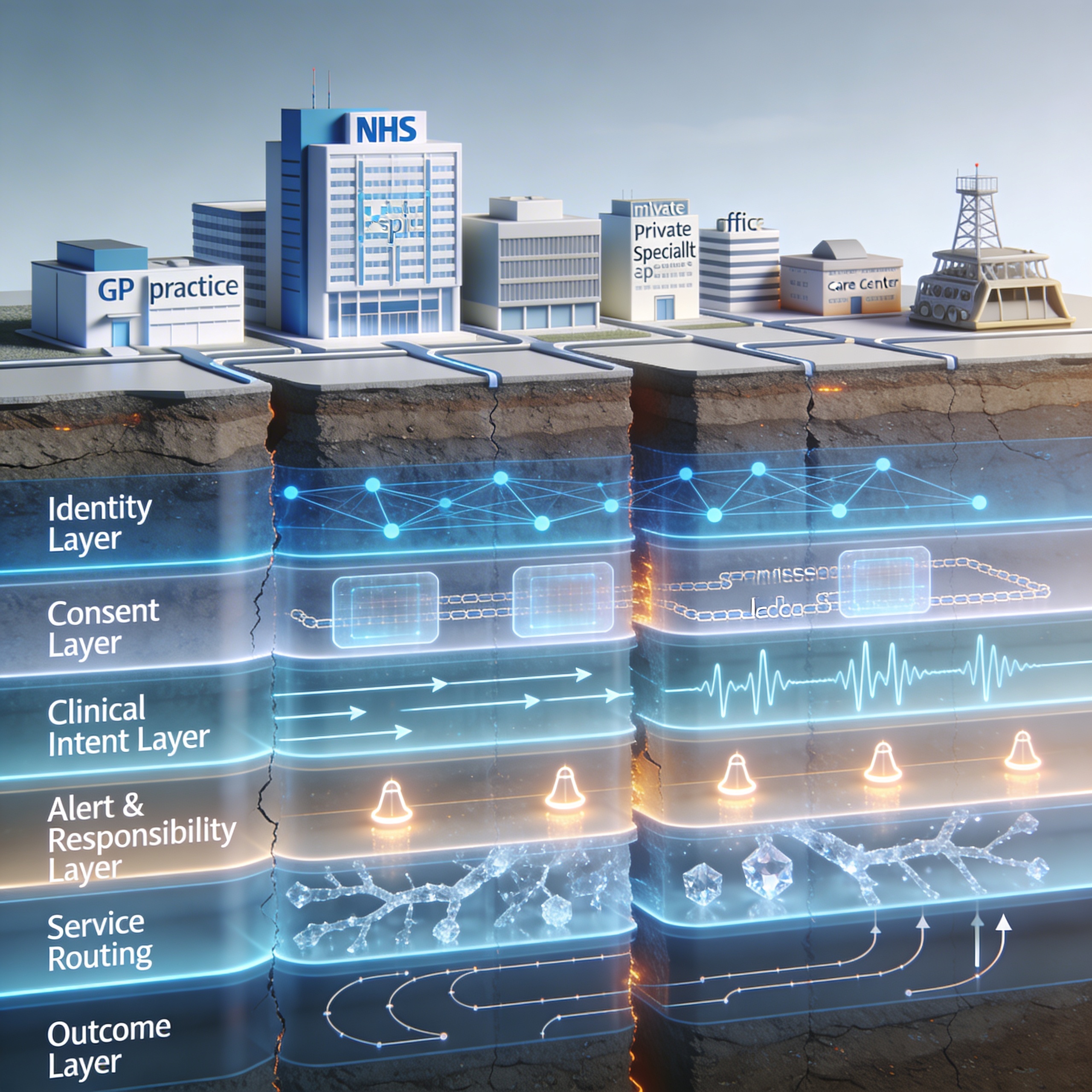
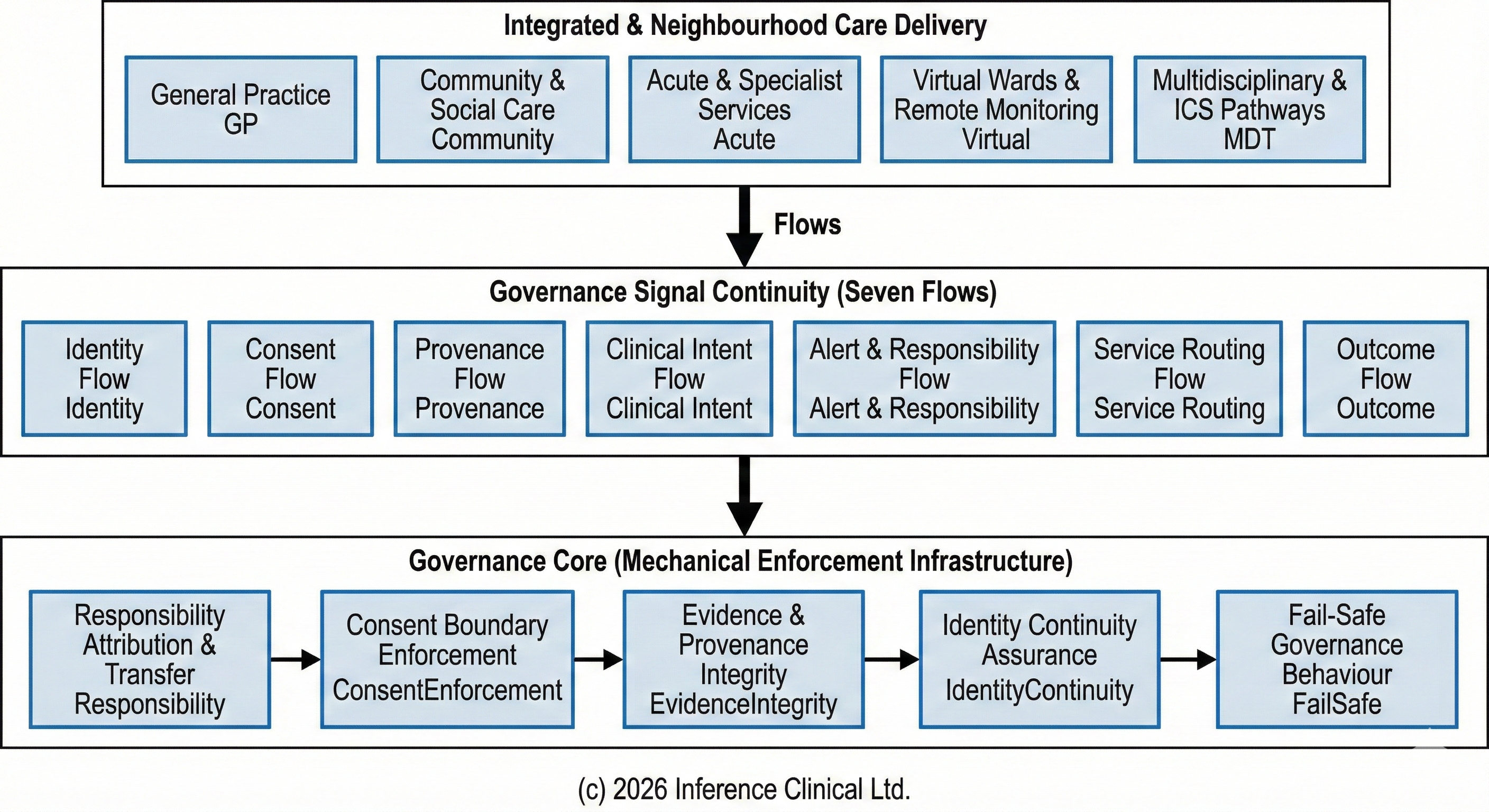
Architecting for Neighbourhood Health: Mapping the Seven Flows in a Neighbourhood Health Centre
The Seven Flows framework defines what must function at every organisational crossing — Identity, Consent, Provenance, Clinical Intent, Alert & Responsibility, Service Routing, and Outcome — and why mapping comes before service design.
Architecting for Neighbourhood Health: What the Implementation Programme Is Missing
The neighbourhood health model multiplies organisational boundaries within a single building. Co-location changes the experience but not the legal architecture. The governance conversation is about structure — the gap is about boundaries.

70% of NHS Digital Health Has No Safety Assurance — And the Boundaries Are Worse
14,747 active digital health deployments across 239 NHS organisations. 70.1% have no documented clinical safety assurance. But the real risk is at the boundaries — where no framework assesses what happens between organisations.

The Constitutional Problem in Healthcare Data Sharing
Healthcare data sharing isn't blocked by technology — it's blocked by constitutional authority. The Constitutional Transition Matrix reveals why cross-domain governance fails and what infrastructure would make it work.
When Your Patient Becomes Nobody's Patient
For 90 hours after a Friday discharge, a patient had no named responsible clinician. MVRT failures are structurally embedded across seven healthcare boundaries — and the system is designed to not notice.

The Governance Gap in the NHS Ten Year Plan & Reforms
The NHS Ten Year Plan creates more organisational boundaries, not fewer. Why boundary governance is the missing layer — and what the Seven Flows methodology reveals about the structural gap.

Minimum Viable Responsibility Transfer
Five structural conditions that must hold before clinical responsibility can safely cross any boundary. From aviation sector handovers to NHS care transitions.

The Handover That Never Happened
Why responsibility dissolves at NHS organisational boundaries — and disappears entirely at constitutional ones. The gap between NHS Act 2006 and Care Act 2014 that no system is watching.
Governance Must Be Executable: Building Infrastructure for Accountability
As NHS integrated care and neighbourhood health models distribute responsibility across organisations, governance must become enforceable infrastructure — not just documentation.

When Safety Becomes Machine Authority
Why training isn't enough — and why the hardest decisions in clinical safety are the ones we automate. How aviation, rail, and healthcare handle the shift from administrative to engineering controls.

The Architecture of Trust
Why clinical governance can't stay procedural — and what Minimum Viable Responsibility Transfer means for healthcare infrastructure. Examining how aviation, finance, and rail solved the same problem.
Mind the Gap #4 — Evidence Decays Faster Than We Admit
Healthcare has plenty of data. What it lacks is durable evidence — evidence that can survive time, organisational change, and scrutiny without being reinterpreted through hindsight.
Mind the Gap #3 — Responsibility Is the Thing Nobody Can Point To
There's a question that surfaces in almost every serious incident review: who was actually responsible at that point? Responsibility is inferred from context, assumed based on role, and socially negotiated.

Mind the Gap #2 — Handoffs Aren't Moments. They're Risk Surfaces.
Most people think of handoffs as moments. A discharge happens. A referral gets sent. Done. That's not how it works. Handoffs are risk surfaces with area, exposure time, and boundary conditions.

Mind the Gap #1 — Care Doesn't Fail Where You Think It Does
Healthcare failures rarely look like failures at the time. They occur in the gaps between decisions, during transitions when accountability becomes ambiguous. Everyone acts reasonably. Everyone is wrong.

Left of the Regulator: Why Operational Maturity Comes Before Clinical Value
Clinical value requires operational maturity. Before regulatory approval matters, before outcomes can be measured, the infrastructure must be solid. Getting the sequence right changes everything.
What the NHS 10-Year Plan Actually Means for Private Medical Insurers
The structural shifts in NHS policy don't just affect providers. Three changes fundamentally alter how insurers must operate: the end of information asymmetry, compliance contagion from PSR, and the prevention evidence gap.
Three Regulatory Shifts Private Healthcare Cannot Ignore
The NHS 10-Year Health Plan changes the operating environment for private providers and insurers. Interoperability mandates, provider selection evidence requirements, and compliance-attached capital demand attention now.
The Hidden Hazard in Neighbourhood Health
NHS neighbourhood health transformation creates fractal boundary problems across ICS, provider, and NHS-private interfaces. How do we govern care that crosses organisational edges?
The Seven Flows of Care: A 4W1H Narrative
Understanding the foundational information flows that enable safe, effective healthcare delivery: Identity, Consent, Provenance, Clinical Intent, and more.
Standing Up Our Live Clinical Safety Mesh
Our safety intelligence environment is now running in real conditions. Not finished, but live enough to observe, test, and learn from.
COSE — The Quiet Layer That Keeps Trust Intact
Clinical data doesn't stay in one place. How COSE makes trust portable in distributed healthcare systems.
FHIR at the Edge
Community-led healthcare needs flexible, local-first digital infrastructure. How FHIR at the edge enables autonomy without fragmentation.
AI Readiness in Health Data Platforms
As AI becomes central to healthcare, platforms will be judged on how ready their data is for safe, explainable, regulatory-grade AI use.
When the Network Sleeps
Healthcare systems must cope with absence and silence. Designing resilient architectures that maintain trust during device dropouts.
From Data Foundations to Clinical Confidence
Flexible, distributed, patient-first data architectures enable trusted AI at scale. How FHIR Cube provides the foundation for interoperable innovation.
Explainability and Auditability in Clinical AI
Turning the Safety Case from a PDF into a Live Control. For executive and management leaders across NHS and provider organisations.
A Strategic Review of the LFPSE Service
With NRLS decommissioned, LFPSE is now mandated for patient safety events. The real challenge is rebuilding reporting culture.
From Waiting Room to Ward
The perspective of general practice is missing in too many digital conversations. Yet GP surgeries are the front door to the health system.
GPs Spend Too Much Time on QOF
How modern health data infrastructure and FHIR can automate QOF tracking, saving GP practices time and protecting vital income.
Engineering Notes — Week 1
Engineering in safety-critical domains has a way of humbling you. This week's focus: reaching full Core-5 rule coverage.
Connecting the Dots
A GP's practical vision for enhanced clinical efficacy through better information systems and local innovation.
Freeing the CSO
How routine compliance issues trap Clinical Safety Officers in endless cycles, and how DCB CoLab transforms CSOs into catalysts for safe innovation.
Enabling the Innovators
How we're creating the infrastructure to help developers and innovators navigate NHS compliance and bring their solutions to healthcare.
Building Distributed Health Data Systems
A comprehensive guide for buyers evaluating distributed health data systems, covering governance, consent, resilience, and implementation.
Why We're Building Inference Clinical
The journey into building Inference Clinical — transforming thirty years of experience into platforms that make NHS innovation easier and safer.
AI and the Future of Consulting and Healthcare
How AI is transforming consulting and healthcare from supply-side models to engagement-driven futures.
Patients and Clinicians at the Heart of Transformation
True NHS digital transformation happens only when patients and clinicians are at the heart of change. Technology should serve people.
Foundations First
Safer NHS digital health starts with stronger foundations. Too many pilots stall because safety, evidence, and governance are left until late.
Building Bridges Between Engineers and Clinicians
How engineers and clinicians can work together to safely deliver community healthcare through shared frameworks, patience, and data flow.
The Messy, Beautiful Challenge of Processing Wearable Signals
The engineering challenges of transforming noisy wearable signals into medical-grade data — from motion artifacts to clinical validation.
Building Preventative Health Together: Samsung
How Inference Clinical's collaboration within Samsung's Health ecosystem supports UK prevention, remote monitoring, and safer digital foundations.
Towards Clinical Software Safety Enablement
How Clinical Software Safety Enablement transforms medical device evaluation, making safety integral to digital health innovation.
Community Care, Proactive by Design
How practices move from reactivity to proactivity: earlier sight, safer data, kinder language, and tech that respects reality on the ground.
Engineering at the Heart of Safer Digital Health
Healthcare tech has been a closed shop for too long. We're changing that by providing guardrails, knowledge, and community.
Beyond Compliance: Clinical Safety as Innovation's Foundation
When clinical safety processes become strategic enablers rather than compliance hurdles, NHS trusts can deploy innovations 70% faster.
The Birth of Inference Clinical
Why we exist: a personal origin story turned practical mission for safer, smarter NHS innovation.